MedHub recently published two posts recapping the webinar “Learnings from a large-scale implementation pilot of the Association of American Medical Colleges (AAMC) Core EPAs.” The webinar featured insight from the renowned Dr. Jonathan Amil, professor of psychiatry and senior associate dean for innovation and health professions and education at Columbia University. In the webinar, he discussed a pilot program in which around a dozen medical education institutions worked to integrate 13 core entrustable professional activities (EPAs) that graduates should perform without direct supervision on their first day of residency. “Entrustable Professional Activities (EPAs) were chosen as the framework for the guidelines because they offer a practical approach to assessing competence in real-world settings and impact both learners and patients,” said the American Association of Medical Colleges.
The first post summarized the core EPAs, the context, structure, and timeline of the pilot, while the second post presented core findings of the pilot. In this post, we’ll uncover the implications of the pilot study – and how they can impact medical education institutions.
The pilot aimed to provide expectations for both learners and teachers that include 13 core EPAs that medical students should perform upon entering residency. It revealed key performance gaps (and opportunities) at the transition point between medical school and residency training.
The findings
Overall, the pilot study shed light on improving the transition from undergraduate to graduate medical education. Dr. Amil summarized the findings into clusters:
Satisfied Core: Cluster A
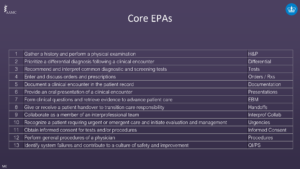
EPAs 1, 2, 5, 6, 7, and 9 (Gather a history and perform a physical examination, prioritize a differential diagnosis following a clinical encounter, document a clinical encounter in the patient record, provide an oral presentation of a clinical encounter, form clinical questions and gather evidence to advance patient care, and collaborate as a member of an interprofessional team) align well with existing curricula, meaning that there exist ample opportunities for learners to practice them with direct observation and feedback.
Calls for Improvement/More Data: Cluster B
EPAs 3, 4, and 8 (Recommend and interpret common diagnostic and screening tests, enter and discuss orders and prescriptions, and give/receive a patient handover to transition care responsibly) that may be represented most prominently in the senior UME curricula, where learners have limited opportunities to practice them with supervision that may be inconsistent or not sufficiently intentional to collect evidence robust enough to substantiate entrustment decisions.
Aspirational EPAs: Cluster C
EPAs 10, 11, 12, and 13 (Recognize a patient requiring urgent or emergent care and initiate an evaluation and management, obtain informed consent for tests and procedures, perform general procedures of a physician, and identify system failures and contribute to a culture of safety and improvement) that in most of our participating schools’ UME curricula appear to be absent or underdeveloped. These EPAs call for improvement.
Cluster D: Calls for Innovation
Telemedicine, discharge planning, and patient-centered decision-making are EPAs that were not included in the originally published list that are nevertheless core to the medical student role and may be considered for inclusion in curricula.
Other insights
The webinar shed light on other ideas as well, like:
- Guiding principles can help with design, communication with learners, and program evaluation.
- There is a need for managing and visualizing data for learners and coaches/advisors.
- Systems need to be flexible enough to accommodate new competencies and frameworks.
- Competency frameworks may shift, thus resources should be flexible.
- Changes in leadership, and pandemics, can impede the adoption of implementing core EPAs. Thus, educators need to be forgiving of the fact that external things can impede goals.
Conclusions on student assessments
As it relates to empirical data with the core competencies and guiding principles, the AAMC concluded the following about student assessments:
- They need to be based on the authentic roles of learners. If educators are assessing learners on a path where they’re not entrusted with a clinical setting, they’re doing something inauthentic and may not be generating valid data.
- They should be based, in part, on direct observation. It’s hard to discern a medical student’s knowledge from how they initially presented it. So, directly observing the performance of skills is important for educators. The assessment is valuable for learners and educators to ensure there is sufficient construct validity.
- They should be consequential to both learners and educators.
- They should contribute to longitudinal data collection.
- They should be fair and equitable; and if not, there will be consequences.
Want more support for entrustment activities?
If you’re an educator looking for more support in tracking student EPAs, look no further than MedHub. Take a look at our success stories to see how they can benefit your institution.
Watch the Full Webinar
About Jonathan Amiel, M.D.
Jonathan Amiel, M.D. is a Professor of Psychiatry and Senior Associate Dean for Innovation in Health Professions Education at Columbia University’s Vagelos College of Physicians & Surgeons. He is also an Attending Psychiatrist at New York Presbyterian and the New York State Psychiatric Institute. Dr. Amiel obtained his bachelor’s degree in biology from Yale University and his MD from Columbia.
He is the past chair of the Association of American Medical Colleges (AAMC) Organization of Resident Representatives and Northeast Group on Educational Affairs and leads its Core Entrustable Professional Activities pilot. He serves on the Advisory Committee for the Gold Humanism Honor Society and chairs its Membership Committee. Dr. Amiel’s work focuses on competency-based education and its relationship to the development of health professionals’ identities. In his work, he partners with educators across the medical school, medical center, university, and colleagues in national and international professional societies to advance the training of health professionals to optimally meet the evolving needs of the public. The overarching goal is to ensure that training is intentional, just, and aligned with public health needs – including developing our next generation of clinician-scientists, educators, and advocates.